Fibroids are benign tumours of the uterine muscle and are unlikely to become malignant. They are most common in childbearing age and their incidence increases with age so that, for example, they will be found in about 40% of women at age 40. In most women, fibroids will not cause any symptoms at all.
The growth of fibroids depends on estrogen, the hormone secreted during the fertility age, and therefore most symptoms will disappear in menopause and even some of the fibroids will decrease in size.
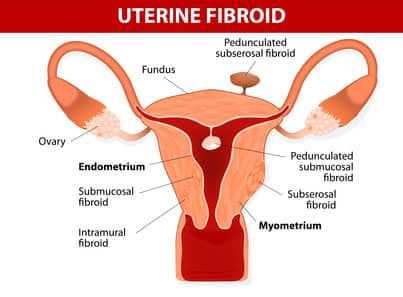
The fibroids can grow anywhere in the womb – inside the cavity, inside the uterine wall or on the uterus, on its outer walls (sub-serous). The symptoms caused by the fibroids depend on their location and size.

Who is at risk for fibroids?
- A woman who has at least one pregnancy that lasts longer than 5 months has a reduced risk of developing fibroids.
- Use of oral contraceptives protects and reduces fibroids risk.
- Ethnic background – fibroids are 2-3 times more common in women of African origin than in white women.
- Obesity is a risk factor for the formation of fibroids.
What are the symptoms associated with the fibroids?
Most fibroids are small and do not cause any symptoms. When there are symptoms, they are related to the number, size, and location of the fibroids in the womb. Common symptoms include:
- Excessive bleeding – heavy bleeding, prolonged periods, bleeding between cycles.
- Pressure in the pelvis and pain – pressure on the bladder or intestines that cause frequency.
- Pain during menstruation.
- Fertility problems and complications during pregnancy.
Which fibroids should be treated?
- Large fibroids that cause pressure on internal organs – bladder, intestines.
- Fibroids that grow at an accelerated rate.
- Fibroids causing abnormal bleeding.
- Fibroids that cause fertility problems.
How to treat fibroids?
There are currently several treatment options that we personally adapt to the patient according to her age, her desire for fertility, location, number and size of fibroids.
Treatments are divided into therapeutic, surgical and radiological.
Drug treatments
birth control pills, injections to stop menstruation – are usually ineffective over time, and after stopping them there is the accelerated growth of the fibroids.
Esmya – A medication designed to shrink fibroids, with an efficiency of 70%, will hopefully be back on the shelves soon.
Mirena IUD
A limited effectiveness. A contraceptive device which contains and secrets a hormone called progesterone, which opposes the estrogen activity, that thrives the fibroids. It is reserved for women with fibroids in the uterine cavity or wall, who approach menopause and wish to maintain their uterus.
Operative hysteroscopy
An operative method in which an optic fibre is inserted under anesthesia through the cervix into the uterine cavity, and by an electrical loop, the fibroid is excised. Is limited to intrauterine fibroids, up to 4-5 cm size.
Surgical laparoscopy
Minimally invasive procedure. Through tiny holes in your tummy, under general anesthesia, optical fibres are inserted and a number of instruments are used for myomectomy.
It is usually suitable for one fibroid, with a diameter of up to 6-7 cm in anterior position on the uterus, on a stalk or protruding towards the abdominal cavity (sub-serous). The procedure is reserved for women who have symptoms of constipation or urinary incontinence, and wish to preserve their uterus without performing open abdominal surgery.
Catheterization and obstruction of the uterine arteries (embolization)
A relatively innovative procedure in which catheterization of the uterine arteries is carried out under x-rays, and releases microscopic particles that block the blood supply to the fibroid. It is especially suitable for fibroids which cause excessive bleeding, intrauterine and/or sub-serous. The method has up to 85% success in reducing the amount of bleeding, with few complications. This method is good for women with previous uterine surgeries and women who are interested in uterine preservation. There is no impediment to conceiving afterwards, but the action is not intended for women who plan another pregnancy for fear of complications of pregnancy and childbirth.
Focused ultrasound
A procedure in which external heating of the fibroid is performed by sound waves under magnetic resonance imaging (MRI), without the need for anesthesia. The procedure is effective for intrauterine wall and/or sub-serous fibroids, with a success rate of about 80%. The treatment is intended for any woman suffering from hemorrhage, regardless of age or family planning.
Laparoscopic hysterectomy
in cases where the woman has several types of fibrosis and completed her family planning. This approach is limited by the size of the uterus and the location and size of the fibroids.
Through tiny holes, similar to myomectomy, the uterus can be excised with or without the uterine cervix, without opening the abdominal wall. A short hospitalization time of 24- 48 hours is usually followed by a quick recovery of 10-14 days and excellent cosmetic results.
Open hysterectomy/myomectomy (the classical approach)
This approach involves the opening of the abdomen and excision of the fibroid or uterus with or without the cervix. Hospitalization time 48-72 hours, recovery at 4-6 weeks and less desirable cosmetic results. This approach is usually reserved to: a woman who underwent previous abdominal surgery, whose fibroid is more than 10 cm in diameter, the uterus is large reaching the belly button or is suspected of malignancy.